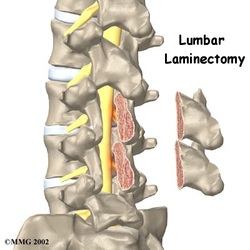
Laminectomy
- Laminectomy is the traditional and most common procedure for lumbar disc disease
- May be performed to relieve the pressure of spinal stenosis (narrowing of the spine) on the spinal cord or spinal nerves or for herniated disc
- Laminectomy is a procedure to surgically excise part of the posterior arch of the vertebra (referred to as the lamina). This allows the surgeon to gain access to part of or all of the protruding disc
- Laminectomy begins with deep tissue dissection, and, as with discectomy, localization is confirmed with x-ray
- Bony removal is commenced, the amount of bone removed depends on the amount of stenosis
- The lamina is thinned with a drill prior to removal, the spinal canal is carefully decompressed
- The wound is irrigated and closed
- A drain may be utilized
http://www.eorthopod.com/content/lumbar-laminectomy
Please use the following link to access a video on laminectomy: http://www.youtube.com/watch?v=EvQPZxXr3Rs
laminectomy retractor from http://www.bsbro.com/product.detail.php?page=155&pID=2052
Post operative nursing care of the laminectomy patient
Care of the laminectomy patient is similar to care of the discectomy patient; regular observation of the patient is necessary as well as pain management and wound and drain care are essential.
BASIC OVERVIEW OF CARE
OBSERVATION
A baseline set of observations should be performed on the patients arrival to the ward and throughout their stay in hospital as per protocol. These observations include:
Neurovascular assessment:
This involves checking the patients limbs for movement and sensation and is performed in a distal and proximal manner below the level of spinal involvement (Harvey 2005). It is important to perform neurovascular observations and to know the patients preoperative deficits so that a baseline can be established and subtle changes can be noted quickly (Harvey 2005). Changes in neurovascular observations may indicate complications including development of spinal cord edema or inflammation of the tissues secondary to damage to motor nerve roots from surgical manipulation. Tissue hemorrhage, compressing the spinal cord may also lead to changes in movement and sensation of the limbs (Doenges et al 2006:262).
Vital observations:
Vital signs need to be monitored frequently to watch for signs of hypovolaemia, including decreased blood pressure and increased pulse rate. Abnormal vital signs such as increased temperature may indicate infection (Harvey 2005).
Pain observation:
Nursing staff can assess patients’ pain by using a verbal numerical scale, zero being no pain and ten being the worst pain imaginable. Increased pain may affect the patients recovery, eg. the patient may be in too much pain to mobilise (Brown et al 2005). The patient may arrive to the ward with patient controlled analgesia (PCA). PCA observations need to be attended as per protocol.
Surgical wound observation:
Nursing staff must also visually check and palpate the surgical site. Change in contour of the surgical site suggests hematoma, or edema formation. Inspection may also reveal bleeding, because vascular injury is a complication of disk surgery; or dura leak of cerebrospinal fluid (CSF) (Doenges et al 2006:262). Redness, heat or abnormal discharge from the surgical site may indicate infection and must be monitored daily (Strayer 2006). The patient should be informed to take measures to reduce strain on the surgical area. This may help to prevent bleeding and haematoma formation in the surgical area. The nurse may need to administer corticosteroids to reduce inflammation of the surgical area in some circumstances, as per the doctor (Ulrich & Canale 2005).
PAIN MANAGEMENT
Acute unrelieved pain may lead to stress, anxiety and fear, impacting on the patients recovery. Immobility related to pain may lead to poor venous return and deep vein thrombosis and the possibility of pulmonary embolism and hypoxaemia. Pain relief is very important for postoperative laminectomy patient, as with other post operative patients. The nurse must implement effective pain control methods including regular pain assessment and pharmacological management as well as the use of non-pharmacological measures. Nursing staff need to make sure the patient has adequate pain relief charted by the doctor. Nursing staff also need to encourage patients to take pain relief regularly to prevent pain from becoming too severe. Inform the patient of side effects of medications (Brown & Edwards 2005).
Patients who undergo lumbar laminectomy might have patient controlled analgesia (PCA) on return to the ward. PCA allows the patient to titrate their own analgesic requirements thus reducing unwanted side effects including sedation, nausea, vomiting and hallucinations (King & Walsh 2007). Additionally, in lumbar laminectomy there are a few non-pharmalogical methods of pain relief the nurse can teach the patient including positioning techniques. The patient should maintain a position that allows the flattening of the lumbosacral spine. This may include slight knee flexion when supine, knees flexed while lying on the side and feet elevated on a foot stool when sitting in a chair. This leads to decreased stretching of the nerves and muscles in the lower back. The patient should avoid sitting or standing for longer than 30 minutes at a time. Patients must be advised not to strain to have a bowel motion and avoid coughing (Ulrich & Canale 2005).
Pain relief that might be prescribed includes:
Non-pharmacological methods of pain relief may include:
URINARY RETENTION AND CONSTIPATION
The postoperative laminectomy patient is at risk for constipation due to swelling and pain around the surgical area; decreased physical activity; lack of privacy; and due to the use of narcotic analgesia. Nursing staff need to administer eperients and educate the patient regarding becoming constipated postoperatively (Doenges et al 2006). Nurses must also be aware that the patient may be at risk for urinary retention. This may be caused by a variety of reasons; indirect sympathetic nervous system stimulation resulting from fear, pain and anxiety; direct stimulation of the sympathetic nerves that innervate the bladder. This may be caused by nerve trauma during laminectomy or inflammation or an accumulation of blood causing pressure on the nerves. Also, decreased perception of bladder fullness may occur with the depressant effect of anaesthesia (Ulrich & Canale 2005).
DRAIN CARE
The wound site must be monitored regularly, see 'surgical wound observation' for further details. As well as this, in laminectomy, often a drain is inserted. Drains are used to prevent the formation of a haematoma or to remove an accumulation of fluid (Walker 2007). If the surgeon has requested for the drain be on suction, the nurse must make sure that it remains on suction, and that the wound drain remains patent. This reduces the accumulation of blood in the surgical area, thus preventing pressure on blood vessels and nerves (Ulrich & Canale 2005). The nurse is also responsible for removal of the drain in most cases. Please see hospital protocol for removal of drains if unsure how to remove. The following website includes a journal article that you may find helpful regarding the safe removal of drains: http://www.snjourney.com/ClinicalInfo/Proced/SurgicalDrainRemove.pdf. The journal article is: "Walker J (2007) Patient preparation for safe removal of surgical drains. Nursing Standard. 21, 49, 39-41."
MOBILITY
The patient will be able to mobilise as per postoperative orders by the surgical team. This is usually the day following surgery; however, if a complication such as CSF leak has occurred the patient may have to remain on bed rest, lying flat, for a period of time depending on the surgeon's preference. The patient may also benefit from a walker if he/she is deconditioned, has difficulty mobilising, or has had a multilevel laminectomy. The patient may benefit from physiotherapy on the ward. Nursng staff, allied health and the surgical team should monitor and assess the patient for the need for rehabilitation, either as an inpatient or outpatient (Strayer 2006).
As with discectomy, the patient should be taught mobilisation techniques eg; when moving out of the bed the patient should be instructed to roll on his/her side and slowly bring the legs over the side of the bed while simultaneously rising up from the torso. This technique minimizes twisting at the waist; minimising pain and stress on the lumbar. Additionally, when standing the patient must use their legs to rise and not push off with the back (Strayer 2006).
DISCHARGE PLANNING
The nurse will need to reinforce to the patient a few strategies for caring for their back and themselves post discharge, these may include:
BASIC OVERVIEW OF CARE
- Observations: neurovascular, vitals, pain and PCA (if the patient has PCA), wound observations.
- Pain management: Administer regular analgesic medication. Encourage the use of PCA and nurse administered analgesia.
- Monitor urine output: potential for retention post op.
- Monitor bowels: administer eperients as needed
- Drain care: monitor for signs of infection. Monitor output. Make sure drain is on suction if requested. Remove when written order by doctor.
- Mobility: Assist the patient when ambulating if necessary, encourage to mobilise as per post operative instructions.
- Discharge: Make sure patient is aware of strategies to care for their back.
OBSERVATION
A baseline set of observations should be performed on the patients arrival to the ward and throughout their stay in hospital as per protocol. These observations include:
Neurovascular assessment:
This involves checking the patients limbs for movement and sensation and is performed in a distal and proximal manner below the level of spinal involvement (Harvey 2005). It is important to perform neurovascular observations and to know the patients preoperative deficits so that a baseline can be established and subtle changes can be noted quickly (Harvey 2005). Changes in neurovascular observations may indicate complications including development of spinal cord edema or inflammation of the tissues secondary to damage to motor nerve roots from surgical manipulation. Tissue hemorrhage, compressing the spinal cord may also lead to changes in movement and sensation of the limbs (Doenges et al 2006:262).
Vital observations:
Vital signs need to be monitored frequently to watch for signs of hypovolaemia, including decreased blood pressure and increased pulse rate. Abnormal vital signs such as increased temperature may indicate infection (Harvey 2005).
Pain observation:
Nursing staff can assess patients’ pain by using a verbal numerical scale, zero being no pain and ten being the worst pain imaginable. Increased pain may affect the patients recovery, eg. the patient may be in too much pain to mobilise (Brown et al 2005). The patient may arrive to the ward with patient controlled analgesia (PCA). PCA observations need to be attended as per protocol.
Surgical wound observation:
Nursing staff must also visually check and palpate the surgical site. Change in contour of the surgical site suggests hematoma, or edema formation. Inspection may also reveal bleeding, because vascular injury is a complication of disk surgery; or dura leak of cerebrospinal fluid (CSF) (Doenges et al 2006:262). Redness, heat or abnormal discharge from the surgical site may indicate infection and must be monitored daily (Strayer 2006). The patient should be informed to take measures to reduce strain on the surgical area. This may help to prevent bleeding and haematoma formation in the surgical area. The nurse may need to administer corticosteroids to reduce inflammation of the surgical area in some circumstances, as per the doctor (Ulrich & Canale 2005).
PAIN MANAGEMENT
Acute unrelieved pain may lead to stress, anxiety and fear, impacting on the patients recovery. Immobility related to pain may lead to poor venous return and deep vein thrombosis and the possibility of pulmonary embolism and hypoxaemia. Pain relief is very important for postoperative laminectomy patient, as with other post operative patients. The nurse must implement effective pain control methods including regular pain assessment and pharmacological management as well as the use of non-pharmacological measures. Nursing staff need to make sure the patient has adequate pain relief charted by the doctor. Nursing staff also need to encourage patients to take pain relief regularly to prevent pain from becoming too severe. Inform the patient of side effects of medications (Brown & Edwards 2005).
Patients who undergo lumbar laminectomy might have patient controlled analgesia (PCA) on return to the ward. PCA allows the patient to titrate their own analgesic requirements thus reducing unwanted side effects including sedation, nausea, vomiting and hallucinations (King & Walsh 2007). Additionally, in lumbar laminectomy there are a few non-pharmalogical methods of pain relief the nurse can teach the patient including positioning techniques. The patient should maintain a position that allows the flattening of the lumbosacral spine. This may include slight knee flexion when supine, knees flexed while lying on the side and feet elevated on a foot stool when sitting in a chair. This leads to decreased stretching of the nerves and muscles in the lower back. The patient should avoid sitting or standing for longer than 30 minutes at a time. Patients must be advised not to strain to have a bowel motion and avoid coughing (Ulrich & Canale 2005).
Pain relief that might be prescribed includes:
- Codeine phosphate
- Oxycodone
- Neuropathic pain medications including gabapentin
- Regular paracetemol
Non-pharmacological methods of pain relief may include:
- Heat packs for spasm or muscular tension
- Ice packs (for no more than 20minutes per hour)
- Position changes regularly
- Gentle massage away from the incision site
URINARY RETENTION AND CONSTIPATION
The postoperative laminectomy patient is at risk for constipation due to swelling and pain around the surgical area; decreased physical activity; lack of privacy; and due to the use of narcotic analgesia. Nursing staff need to administer eperients and educate the patient regarding becoming constipated postoperatively (Doenges et al 2006). Nurses must also be aware that the patient may be at risk for urinary retention. This may be caused by a variety of reasons; indirect sympathetic nervous system stimulation resulting from fear, pain and anxiety; direct stimulation of the sympathetic nerves that innervate the bladder. This may be caused by nerve trauma during laminectomy or inflammation or an accumulation of blood causing pressure on the nerves. Also, decreased perception of bladder fullness may occur with the depressant effect of anaesthesia (Ulrich & Canale 2005).
DRAIN CARE
The wound site must be monitored regularly, see 'surgical wound observation' for further details. As well as this, in laminectomy, often a drain is inserted. Drains are used to prevent the formation of a haematoma or to remove an accumulation of fluid (Walker 2007). If the surgeon has requested for the drain be on suction, the nurse must make sure that it remains on suction, and that the wound drain remains patent. This reduces the accumulation of blood in the surgical area, thus preventing pressure on blood vessels and nerves (Ulrich & Canale 2005). The nurse is also responsible for removal of the drain in most cases. Please see hospital protocol for removal of drains if unsure how to remove. The following website includes a journal article that you may find helpful regarding the safe removal of drains: http://www.snjourney.com/ClinicalInfo/Proced/SurgicalDrainRemove.pdf. The journal article is: "Walker J (2007) Patient preparation for safe removal of surgical drains. Nursing Standard. 21, 49, 39-41."
MOBILITY
The patient will be able to mobilise as per postoperative orders by the surgical team. This is usually the day following surgery; however, if a complication such as CSF leak has occurred the patient may have to remain on bed rest, lying flat, for a period of time depending on the surgeon's preference. The patient may also benefit from a walker if he/she is deconditioned, has difficulty mobilising, or has had a multilevel laminectomy. The patient may benefit from physiotherapy on the ward. Nursng staff, allied health and the surgical team should monitor and assess the patient for the need for rehabilitation, either as an inpatient or outpatient (Strayer 2006).
As with discectomy, the patient should be taught mobilisation techniques eg; when moving out of the bed the patient should be instructed to roll on his/her side and slowly bring the legs over the side of the bed while simultaneously rising up from the torso. This technique minimizes twisting at the waist; minimising pain and stress on the lumbar. Additionally, when standing the patient must use their legs to rise and not push off with the back (Strayer 2006).
DISCHARGE PLANNING
The nurse will need to reinforce to the patient a few strategies for caring for their back and themselves post discharge, these may include:
- Gradually return to activities of daily living and lifestyle
- Avoid heavy lifting for 4-6 weeks postoperatively
- Reinforce no lifting, bending twisting
- No sitting for extended periods for 6 weeks postoperatively (including long car trips)
- Instruct patient to take short walks to avoid excessive fatigue
- Patient must change positions frequently
- Remind the patient not to drive while taking analgesic medications as they may cause drowsiness
- Sexual activity may be resumed 2 weeks postoperatively
- The surgical team should inform the patient of appropriate return to work recommendations
- Nursing staff will need to work with allied health teams to ensure the patient will be able to cope on return home. The patient should be able to make alternate arrangements in regards to everyday living activities including vacumming and laundry. Services including child care and cleaning services should be made available to patients who may not have support systems available to assist postoperatively.
- Assess the patients need for rehabilitation or outpatient physiotherapy
- The patient should be discharged with adequate analgesia eg, oxycodone
